
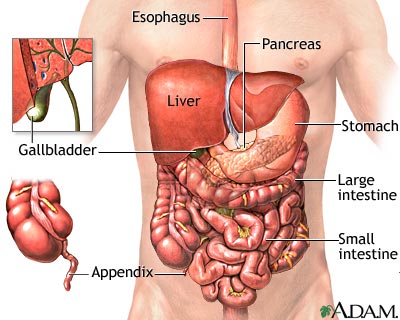
Our abdomen is divided into two cavities: peritoneal and retroperitoneal cavity. In the peritoneal, our liver, stomach, spleen, gallbladder, and small intestine are located. In the retroperitoneal cavity, our kidneys, ureters, and large intestine are located.
Our abdomen contains our digestive organs, and reproductive organs. So, if a knife is penetrated into the abdomen, and it lacerates our stomach, their is now a build up of chemicals entering the peritoneal cavity. These chemicals, will actually start to digest our tissues, thus causing more harm. If our intestines are lacerated, than their will be a buildup of bacteria in our peritoneal cavity, again causing more harm by "eating" away at our tissues.
Our liver, one of the largest organs in our body, on the other hand, is partially protected by our ribs, and sits more posterior than our stomach, gallbladder, and pancreas. Still, the liver is the most commonly affected organ, caused by penetrating trauma. Any laceration to the liver will cause a massive hemorrhage into the peritoneal cavity. Our liver can bleed over a liter of blood. That is pretty significant, since their is only about five liters of blood in our body.
We also need to remember that our aorta is also in our abdomen. This is important to remember, because as an object is penetrated into the abdomen, it can severe the aorta, causing massive hemorrhaging, leading to patient death.
In the cases where the intestine are protruding out from a laceration, also called evisceration, we want to immediately apply a wet dressing, covered by an occlusive dressing. Never try to push the intestine back in the abdomen, because 1) we will cause all other organs to be shifted, 2) we will be introducing more bacteria into the cavity, and 3) we just don't know what else is going on within the cavity.
All injuries to the abdomen should be considered serious, because it is hard to judge just how bad the damage is. Just because their may be internal bleeding, doesn't mean that the signs will show right away. It takes some time for the discoloration to be noted, as well as distention, but you will be able to see it while in the prehospital setting.
We want to assess these patients quickly, and transport quickly. If their are any objects sticking out from the abdomen, we want to secure the object in place. We never want to remove any objects from the abdomen, as the object could be helping the patient from bleeding out.
If our patient becomes hypotensive, we want to start an IV and titrate the fluids to maintain a systolic blood pressure of 90 mmHg. If we cause an increase in BP, say to 120 mmHg systolic, we cause two issues. 1) As we introduce more fluid into the vascular system, we can dislodge a blood clot since their is now a greater force being pushed against the clot. 2) The patient is bleeding out blood now normal saline. Blood contains the hemoglobin and clotting factors, where NS doesn't. So, by giving NS, we are actually causing an increase in fluid, and not blood, which is really what the patient needs, since they need more hemoglobin to transport oxygen, and clotting factors in order to help form clots to spot the bleeding.
Referred Pain:
Spleen: pain referred to left shoulder
Pancreas: pain radiates to back
Kidneys: pain radiates from flank to groin and hematuria
Liver: pain referred to the right shoulder
No comments:
Post a Comment